CASE20250528_002
Balloon-Assisted Techniques for Managing Failed Perclose Closure During TAVR
By Ju Hyeon Kim
Presenter
Ju Hyeon Kim
Authors
Ju Hyeon Kim1
Affiliation
Asan Medical Center, Korea (Republic of)1,
View Study Report
CASE20250528_002
TAVR - Complex TAVR
Balloon-Assisted Techniques for Managing Failed Perclose Closure During TAVR
Ju Hyeon Kim1
Asan Medical Center, Korea (Republic of)1,
Clinical Information
Relevant Clinical History and Physical Exam
This is a 73-year-old male (height: 162.6 cm, weight: 59.3 kg, BMI: 23.3) presenting with New York Heart Association (NYHA) Class II dyspnea on exertion (DOE).
 2-1.avi
2-1.avi
2-2.avi
Relevant Test Results Prior to Catheterization
Findings show severe aortic stenosis (EOA 0.56cm², gradients 63/41mmHg, Vmax 4.0m/s). LVEF is 28% with biventricular dysfunction and LA enlargement. History includes atrial fibrillation with RVR and prior stroke. PFTs indicate an obstructive pattern (FEV1 64%, FVC 74%, ratio 0.58). STS score is 3.6% (intermediate risk).
Relevant Catheterization Findings
TAVR performed with 26mm SAPIEN 3 valve (Edwards) with excellent deployment and positioning. Predilation completed, valve implanted under fluoroscopic guidance with full expansion and appropriate seating. Post-deployment echo: no paravalvular leak, no AR, no pericardial effusion. Hemodynamics stable with no conduction disturbances or complications.
Interventional Management
Procedural Step
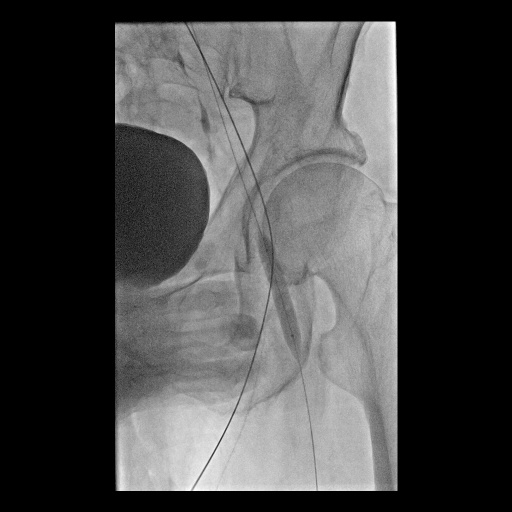
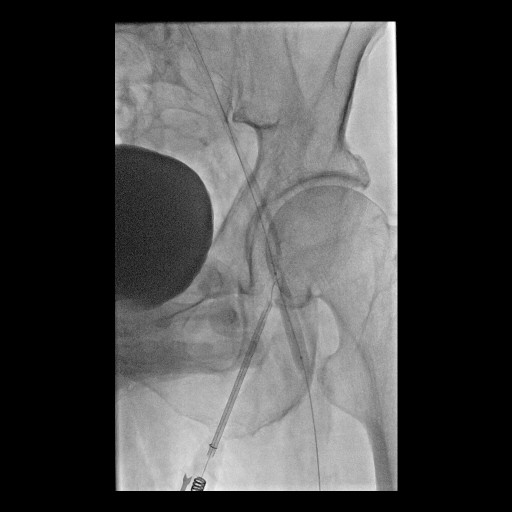
TAVR was performed with a 26 mm SAPIEN 3 valve using left CFA access. The initial Pre-closure closure failed, resulting in left CFA dissection and occlusion. This was managed through a contralateral approach by rewiring the left CFA using an 014 wire and MCT CXI catheter. Balloon tamponade was applied to control bleeding. A subsequent Proglide deployment was performed via the remaining left-side wire, followed by successful hemostasis using a Femoseal device. The procedure concluded without additional complications.
5-4.avi
Case Summary
In cases where initial pre-closure fails, the presence of a large access site created by the TAVR delivery system increases the likelihood of subsequent Proglide deployment failure. However, as demonstrated in this case, a contralateral approach with balloon tamponade can reduce the large access site and enhance the success rate of Proglide reattempts.