CASE20250516_001
The Troublesome Tulip: A Complex Case Report on Transcatheter Atrial Septal Defect Closure
By Wickramasinghe Wasala Mudiyanselage Pasan Aminda B Abeysenevi, Tanya Pereira, Leonard Wanninayake, Nadeeja Seneviratne
Presenter
Wickramasinghe Wasala Mudiyanselage Pasan Aminda B Abeysenevi
Authors
Wickramasinghe Wasala Mudiyanselage Pasan Aminda B Abeysenevi1, Tanya Pereira1, Leonard Wanninayake1, Nadeeja Seneviratne1
Affiliation
National Hospital of Sri Lanka, Sri Lanka1,
View Study Report
CASE20250516_001
Atrial Septal Defect (ASD) Closure - Atrial Septal Defect (ASD) Closure
The Troublesome Tulip: A Complex Case Report on Transcatheter Atrial Septal Defect Closure
Wickramasinghe Wasala Mudiyanselage Pasan Aminda B Abeysenevi1, Tanya Pereira1, Leonard Wanninayake1, Nadeeja Seneviratne1
National Hospital of Sri Lanka, Sri Lanka1,
Clinical Information
Relevant Clinical History and Physical Exam
45-year-old male diagnosed with diabetes mellitus, hypertension dyslipidaemia and an ASD was referred for evaluation of exertional shortness of breath from the endocrine clinic. He did not complain of angina, orthopnoea or peripheral oedema. ASD device closure had failed once. There was no history pulmonary or haematological pathologies. Examination revealed a fixed split of second heart sound. There were no features of pulmonary hypertension or heart failure. Lung auscultation was unremarkable.
Relevant Test Results Prior to Catheterization
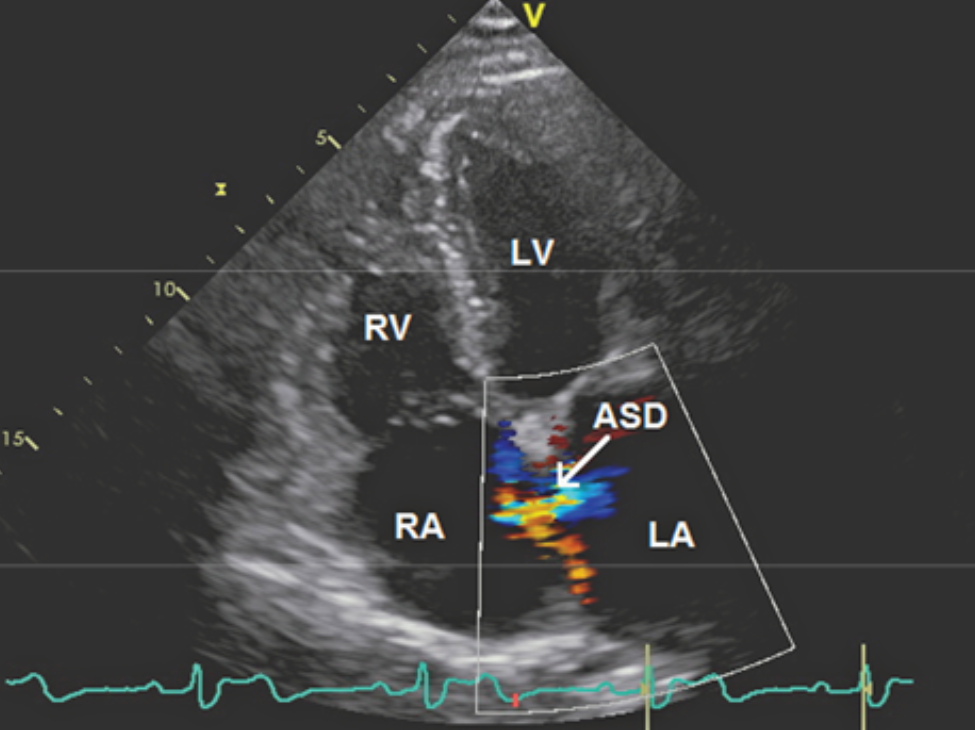
ECG was normal. The transthoracic echocardiogram revealed an ASD with left to right shunt, a TRPG of 30mmHg and RA dilatation. Right and left heart functions were normal. CXR, TSH, haemoglobin, renal and liver functions were normal.Transoesophageal echocardiography revealed an ostium secundum ASD measuring 32 mm. Aortic and mitral margins were deficient with a floppy IVC margin. Septal rims were satisfactory for device closure. Pulmonary venous drainage was normal.
Relevant Catheterization Findings
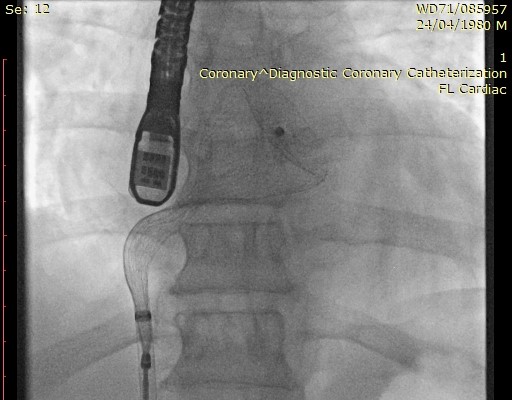
Right femoral venous access was obtained. MPA mean pressure was 35mmHg. A super-stiff wire was placed in left upper pulmonary vein and a 12 F delivery sheath was advanced. Deployment of a 38 mm MemoPart™ occluder was attempted thrice. The device kept falling back into the right atrium. Re-deployment was attempted under TOE guidance. During the process, the left atrial disc exhibited marked concavity and tulip--like deformation.This prevented the device from being re-captured in to the sheath.
 Tulip deformity.mp4
Tulip deformity.mp4
Interventional Management
Procedural Step
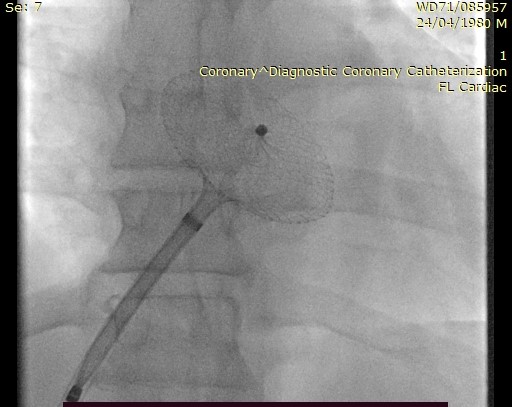
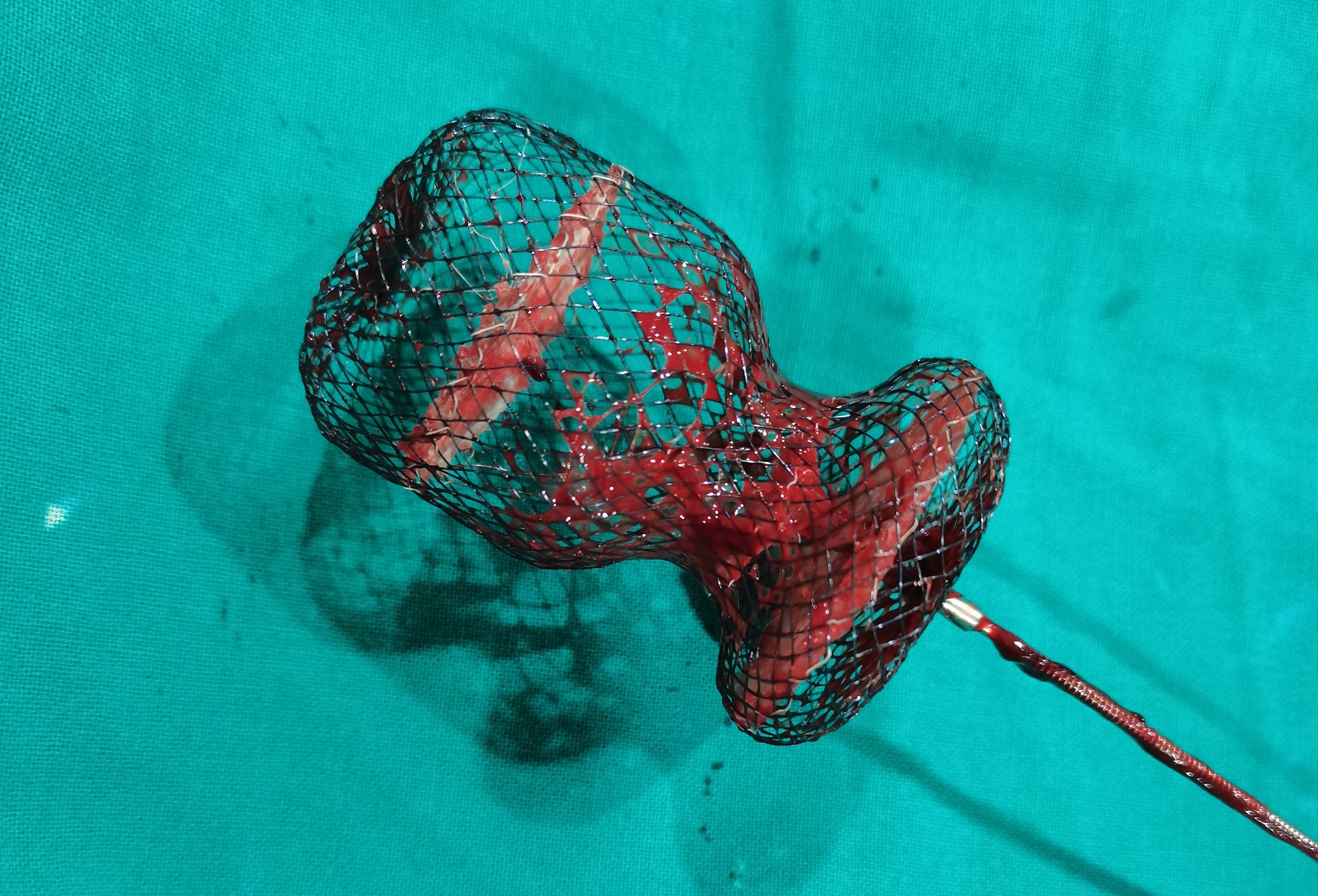
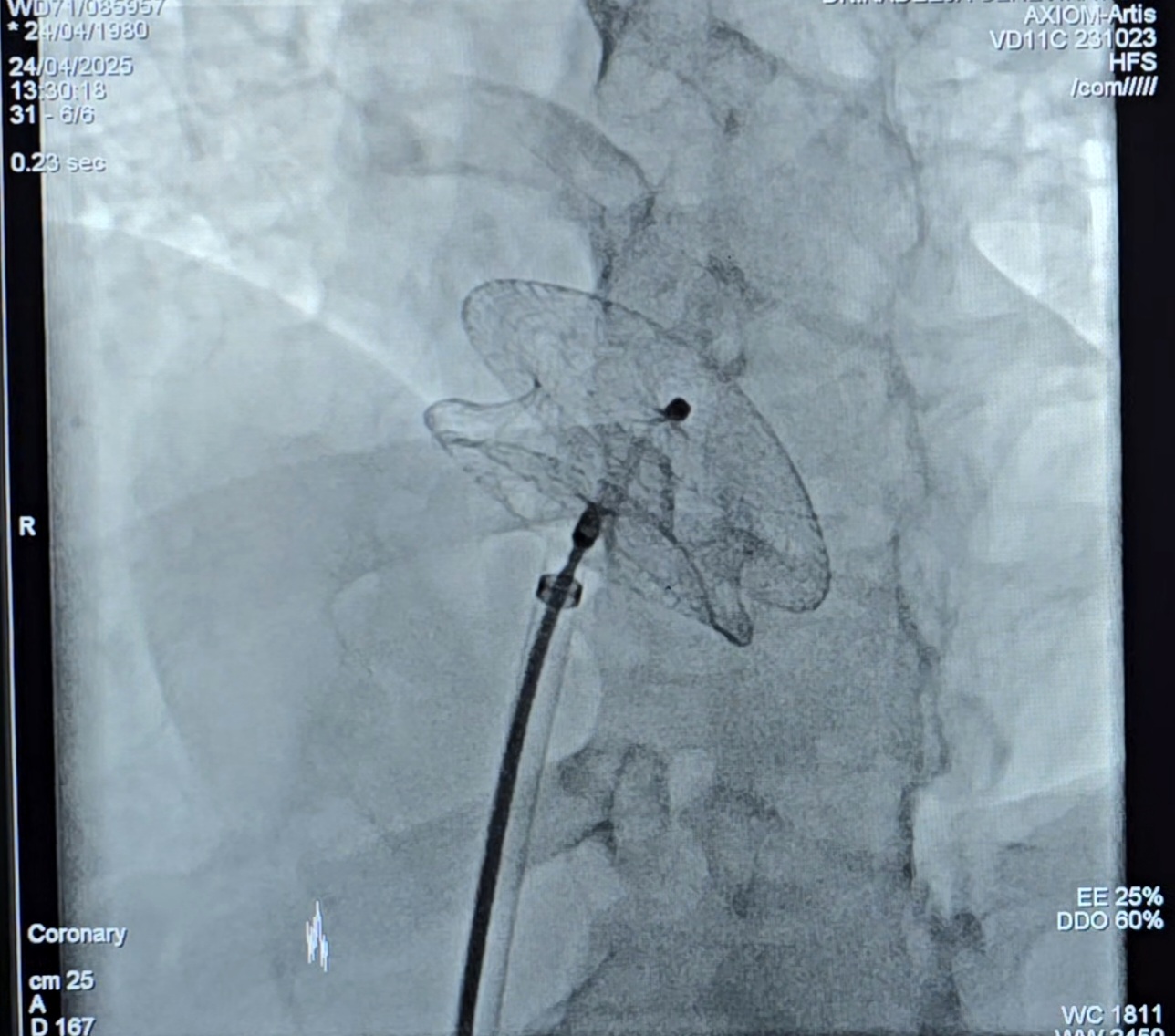
Multiple attempts to recapture the device in to the sheath through femoral access were unsuccessful. The deformity prevented the nitinol sheath from folding in. Larger sheath sizes were not available to be used.Right internal jugular venous access was obtained using a 6 F sheath. A 3-loop snare catheter was advanced via a 6F Judkins Right (JR) catheter in an attempt to snare the knob of the LA disc. This was unsuccessful. Therefore, a 3F COOK vascular retrieval biopsy forcep was advanced through the same JR catheter from above. The strategy was to pull the deformed device upwards and reduce the concavity while pulling the device in-to the sheath from below. After multiple attempts, the LA disc could be grasped and retracted momentarily allowing the recapture of the ASD device in to the sheath.The patient was haemodynamically stable except for a small neck haematoma. It was decided to retry ASD closure with a 34mm MemoPart™ occluder under direct TOE guidance during the same attempt. The super-stiff wire was placed in the right upper pulmonary vein for better alignment of the device.The ASD could be closed successfully. Confirmation of closure was obtained via imaging (fluoroscopy, TTE and TOE).
capturing - final.mp4
Case Summary
ASD device closure offers excellent clinical outcomes with minimal invasiveness. Device-related complications, though rare, can have serious implications. The unique 'tulip malformation’, a concavity and bulbous deformation of the left atrial disc makes retrieval difficult. Mechanical factors such as device stiffness, atrial wall interaction, and incomplete multiple deployments are possible aetiologies. Oversized sheaths, reprocessed devices and device waist twists also contribute. Operator awareness of alternative retrieval strategies is crucial. The value of imaging, early recognition of complications and the importance of situational adaptation in complex procedures should be highlighted.