CASE20250515_004
Valve in Valve TAVR Navigating Through TEVARs
By Christina Mew, Anthony Camuglia
Presenter
Christina Mew
Authors
Christina Mew1, Anthony Camuglia1
Affiliation
Princess Alexandra Hospital, Australia1,
View Study Report
CASE20250515_004
TAVR - Valve-in-Valve TAVR
Valve in Valve TAVR Navigating Through TEVARs
Christina Mew1, Anthony Camuglia1
Princess Alexandra Hospital, Australia1,
Clinical Information
Relevant Clinical History and Physical Exam
A 77-year-old gentleman with severe degenerative bioprosthetic aortic regurgitation presented with acute decompensated heart failure. His history was pertinent for surgical aortic valve replacement with a 29mm Perimount prosthesis 10 years prior and acute type B aortic dissection 4 years prior treated with thoracic endovascular aortic repair (TEVAR) with three thoracic stent grafts, left subclavian artery embolization with coils, and left common carotid bypass grafting.
 Video 1 - 3D Aorta Recon Loop.mov
Video 1 - 3D Aorta Recon Loop.mov
Relevant Test Results Prior to Catheterization
TTE showed 4/4 severe intravalvular aortic regurgitation with LVEF 60%. Mean transaortic gradient was 37mmHg with RVSP of 70mmHg. CT confirmed all three thoracic aortic stent grafts were patent but highlighted extreme tortuosity from the aortic arch to the iliofemoral system (video 1).
Following multidisciplinary assessment, including vascular surgical assessment, Heart Team recommended transfemoral transcatheter aortic valve replacement (TAVR) due to high redo surgical risk.
Video 2 - Iliac tortuosity.mov
Following multidisciplinary assessment, including vascular surgical assessment, Heart Team recommended transfemoral transcatheter aortic valve replacement (TAVR) due to high redo surgical risk.
Relevant Catheterization Findings
Interventional Management
Procedural Step
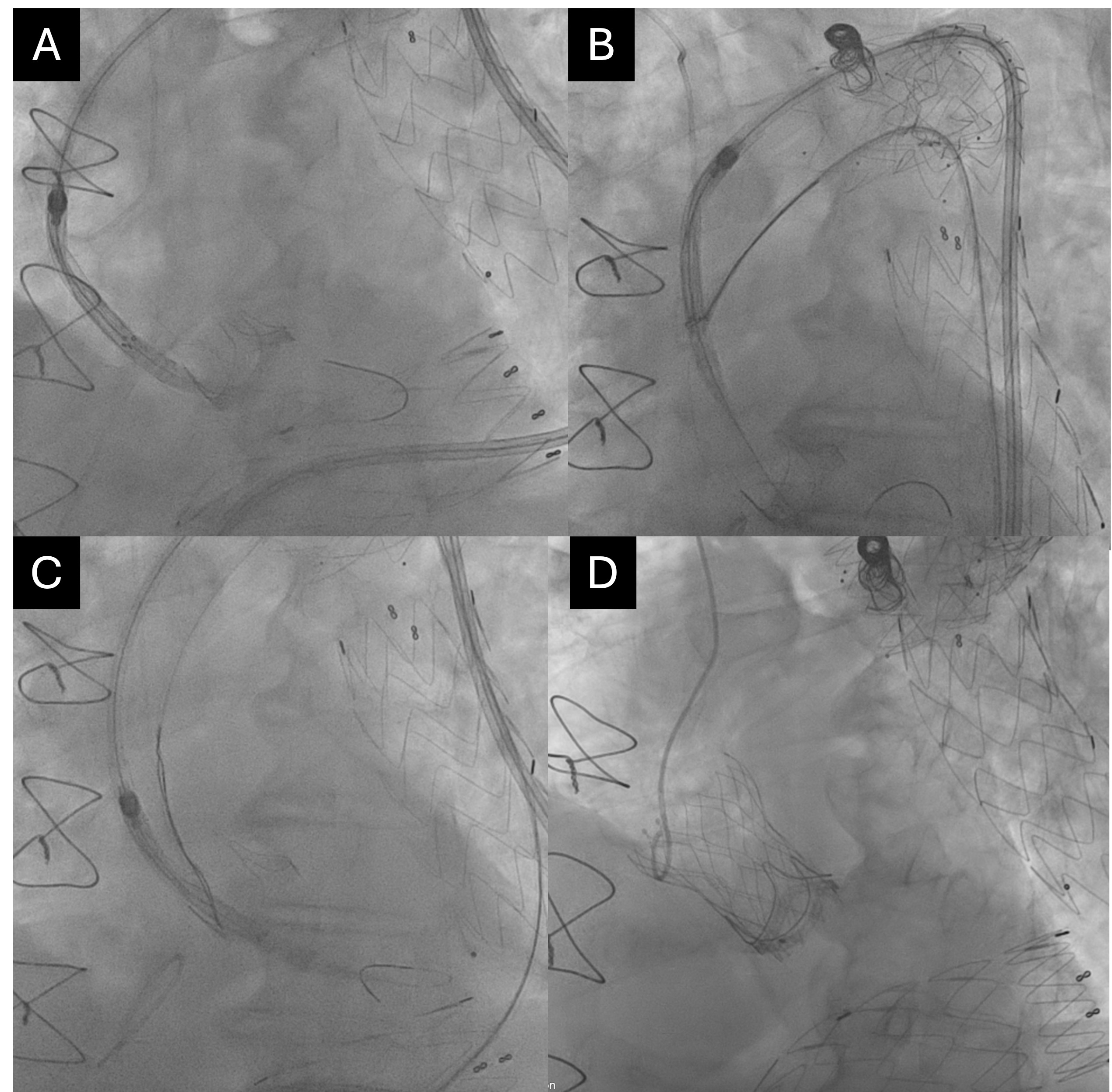
Access was obtained in the left femoral artery. The use of an Amplatz extra stiff wire was required to traverse the iliac system. Delivery of all equipment to the ascending aorta proofed challenging owing to wire bias exacerbated by the thoracic stent grafts and the inherent aortoiliac tortuosity. Despite exchanging the Safari2 for a Lunderquist extra stiff wire, the THV could not be delivered across the surgical aortic valve due to poor coaxial alignment (figure A).
The snare catheter assisted aortic valve crossing technique was utilised. Contralateral femoral access was obtained. The THV was once again delivered over a Lunderquist wire from the left femoral artery but this time through a prepositioned 35mmx120cm Amplatz gooseneck snare from the right femoral sheath. Once in the ascending aorta, the snare was tightened and traction applied to allow centralisation and delivery of the THV across the surgical aortic valve (figure B). Traction applied to the distal portion of the THV allowed valve crossing but the snare became trapped between the two prostheses (figure C). After several attempts of recrossing with the assistance of the snare, a position was ultimately found such that the snare could be removed following valve crossing. The 29mm Navitor self-expandable THV was implanted was implanted and postdilated with a 28mm Valver balloon. The valve in valve THV was well seated (figure D) with no residual aortic regurgitation. There were no complications.
The snare catheter assisted aortic valve crossing technique was utilised. Contralateral femoral access was obtained. The THV was once again delivered over a Lunderquist wire from the left femoral artery but this time through a prepositioned 35mmx120cm Amplatz gooseneck snare from the right femoral sheath. Once in the ascending aorta, the snare was tightened and traction applied to allow centralisation and delivery of the THV across the surgical aortic valve (figure B). Traction applied to the distal portion of the THV allowed valve crossing but the snare became trapped between the two prostheses (figure C). After several attempts of recrossing with the assistance of the snare, a position was ultimately found such that the snare could be removed following valve crossing. The 29mm Navitor self-expandable THV was implanted was implanted and postdilated with a 28mm Valver balloon. The valve in valve THV was well seated (figure D) with no residual aortic regurgitation. There were no complications.
Case Summary
This case allowed the demonstration of the snare catheter assisted aortic valve crossing technique in a patient with challenging transfemoral access due to multiple thoracic stent grafts and extreme aortoiliac tortuosity.