CASE20250509_001
Unmasking the Truth: A Case Study on Cardiac Amyloidosis Presenting with Shortness of Breath
By Dr. Sharadindu Shekhar Roy
Presenter
Dr. Sharadindu Shekhar Roy
Authors
Dr. Sharadindu Shekhar Roy1
Affiliation
National Institute of Cardiovascular Diseases and Hospital (NICVD), Dhaka, Bangladesh., Bangladesh1,
View Study Report
CASE20250509_001
Imaging - Echocardiography
Unmasking the Truth: A Case Study on Cardiac Amyloidosis Presenting with Shortness of Breath
Dr. Sharadindu Shekhar Roy1
National Institute of Cardiovascular Diseases and Hospital (NICVD), Dhaka, Bangladesh., Bangladesh1,
Clinical Information
Relevant Clinical History and Physical Exam
A 57 years old man presented with shortness of breath and generalized swelling of the body for 3 months. Physical examination showed multiple purpuric spots in the back and periorbital region with macroglossia. Pitting ankle edema was present in both legs. JVP was raised. Pulse was 100 beats/minute. BP was 100/70 mm of Hg. Precordial examination revealed no abnormality but bilateral fine crepitation was found in both lower lung fields on auscultation.

Relevant Test Results Prior to Catheterization
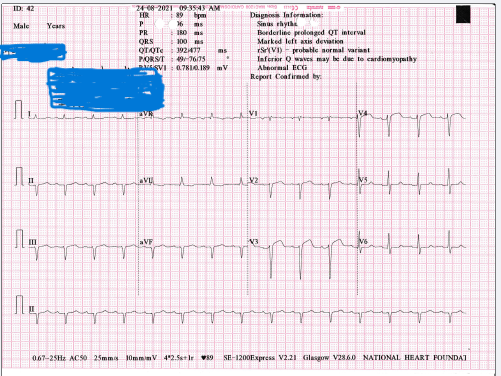
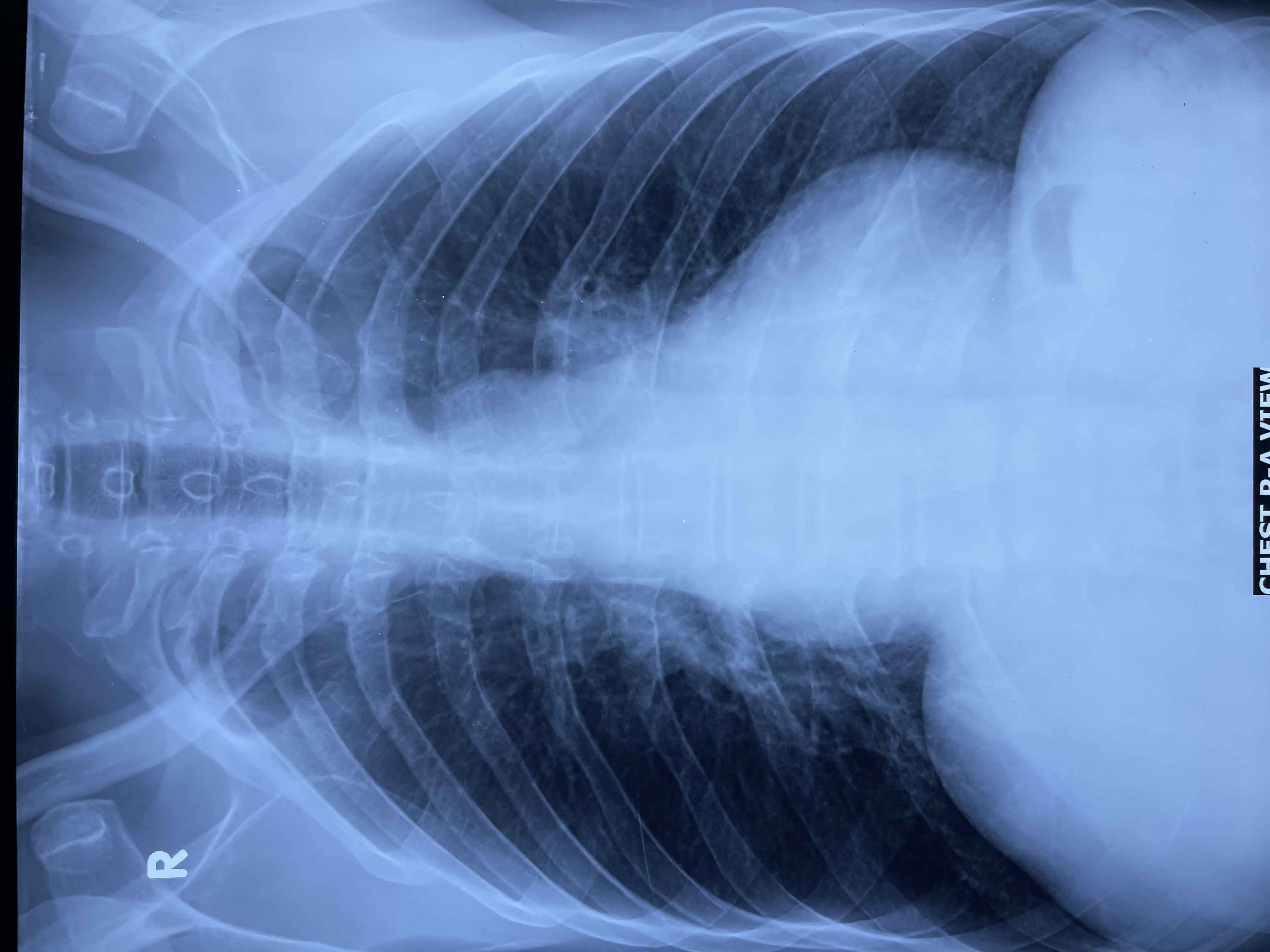
ECG showed low QRS voltage and prominent Q waves in the inferior leads. Chest x-ray revealed mild cardiomegaly. Laboratory tests had shown the normal CBC with CRP 0.26 mg/l, random blood glucose 6.11 mmol/L, serum creatinine 0.9 mg/dL, alanine aminotransferase (ALT) 29.48 U/L and serum albumin 3.9 gm/dL. On urinalysis, specific gravity was 1.020 with trace protein. An abdominal ultrasonography showed moderate ascites and congestive hepatomegaly.
 Echo_Video_ Biatrial Enlargement.mp4
Echo_Video_ Biatrial Enlargement.mp4
Relevant Catheterization Findings
Serum protein electrophoresis was normal, and a urinary Bence Jones Protein was absent. Serum free light chain analysis showed normal free kappa (11.2 mg/L) but significantly increased free lamda (272 mg/L) chain considering the limit for normal individual is up to 19.4 mg/L for free kappa and 26.3 mg/L for free lamda chain respectively. Kappa/ Lamda chain ratio was 0.04 (normal ratio is 0.26-1.65).
Interventional Management
Procedural Step
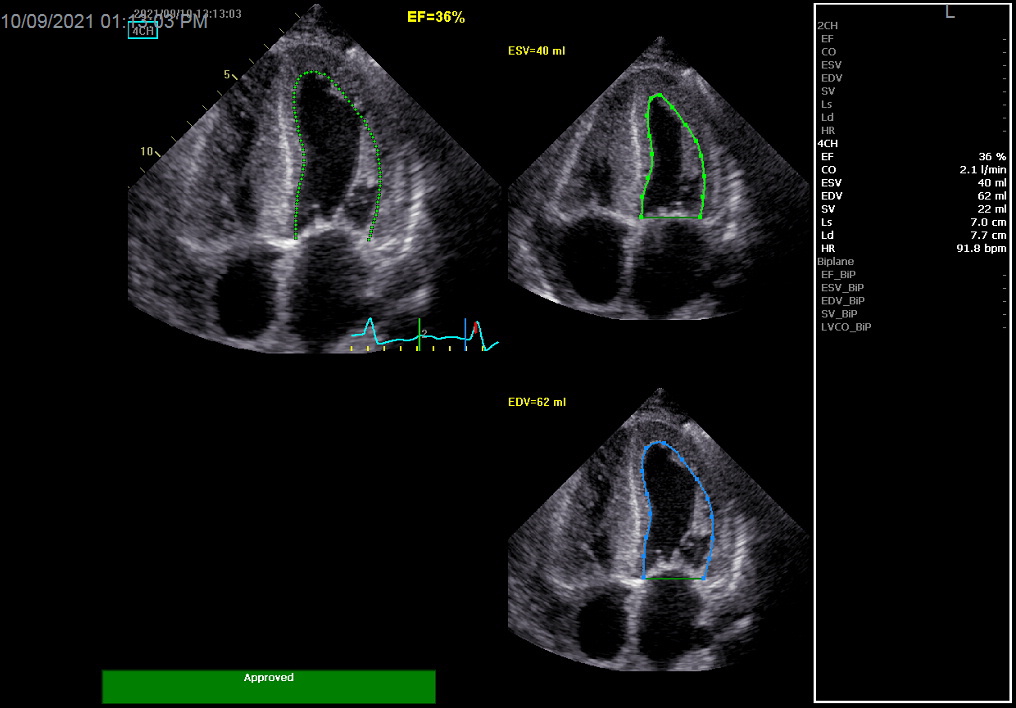
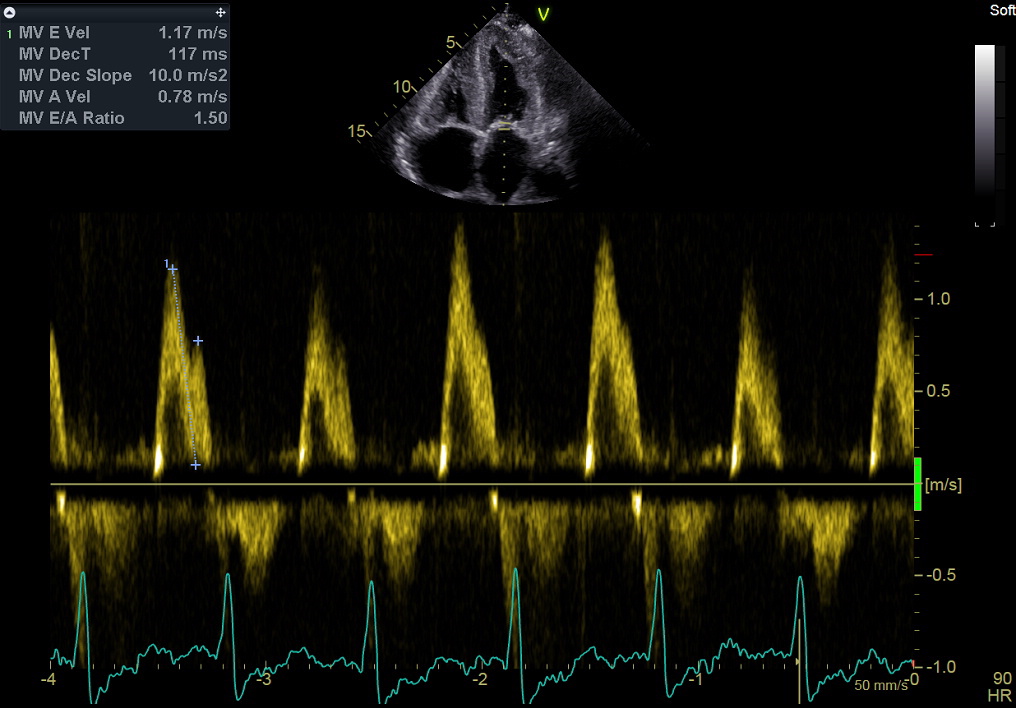
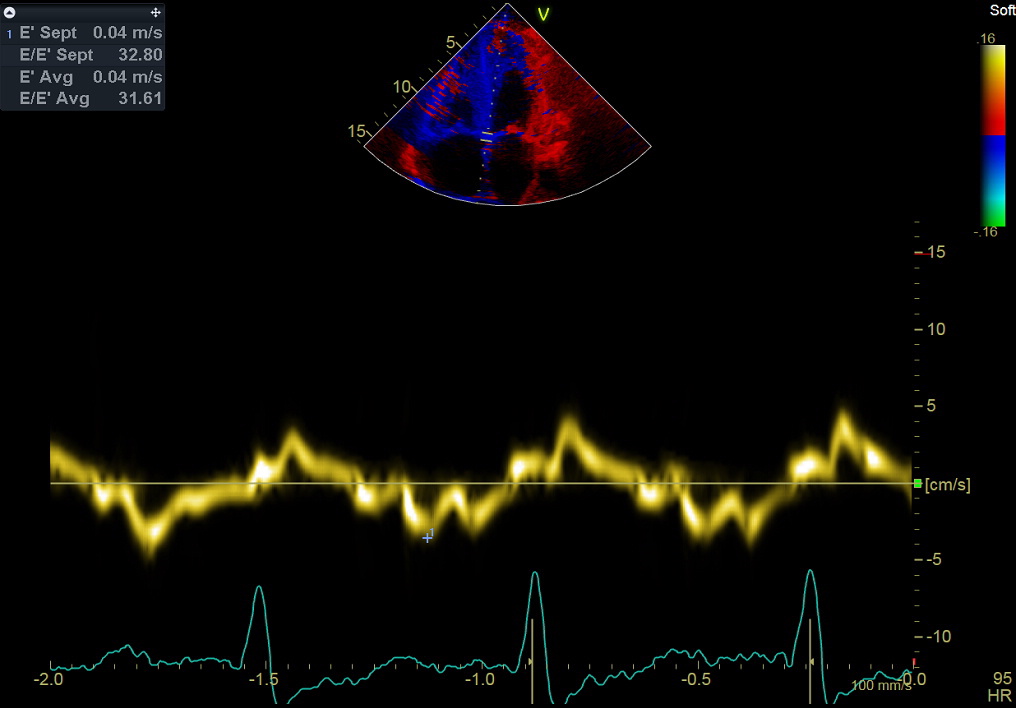
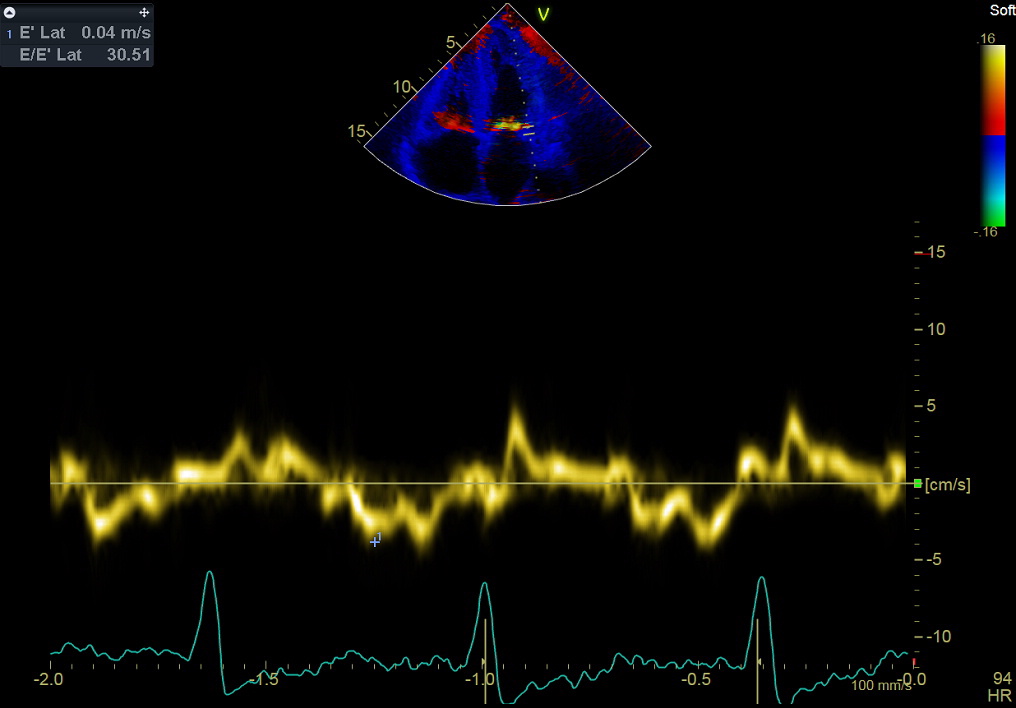
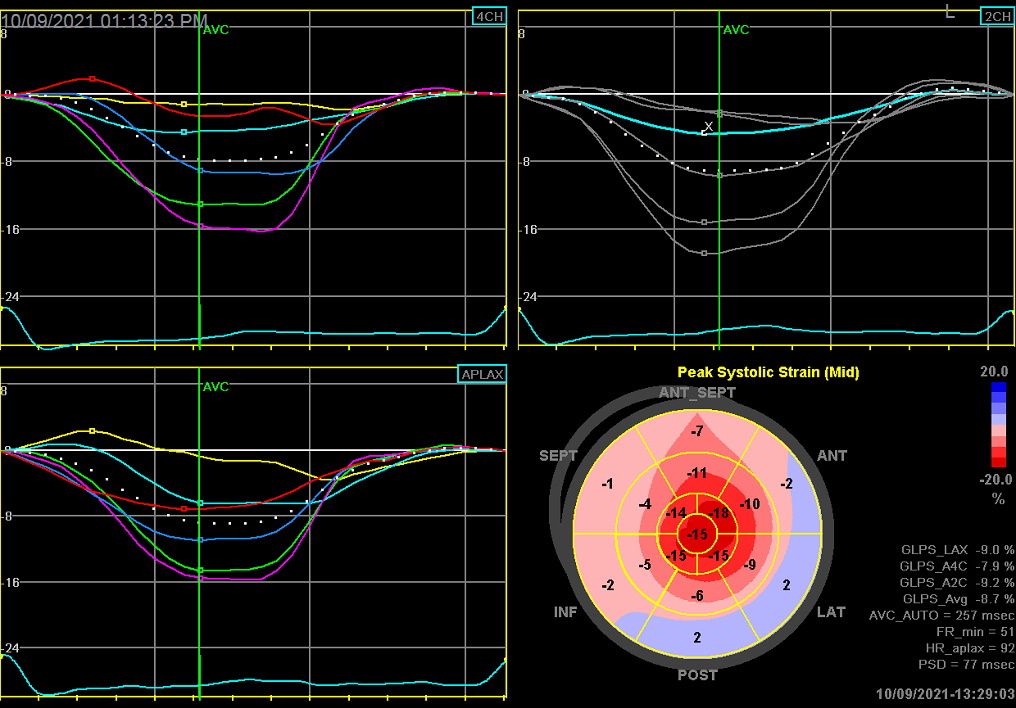
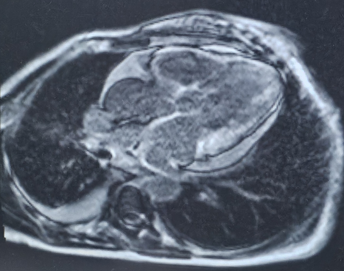
Echocardiography had shown dilated the both atria with left atrial volume index 40 mL/m2. Both ventricles were hypertrophied with hypokinesia of all their segments. Myocardium showed granular appearance. The leaflets of mitral and tricuspid valves were thickened. The cusps of pulmonary and aortic valves were also thickened. Interatrial septum was found thickened. Doppler study showed features of grade-ll left ventricular diastolic dysfunction. Both septal and lateral mitral annular tissue velocity were significantly reduced. Speckle tracking echocardiography showed reduced (- 8.7%) global longitudinal strain of the left ventricle. Apical sparing pattern with 'cherry on top' appearance was noted. Cardiac magnetic resonance imaging (CMRI) showed hypertrophied myocardium with hyperintensity in signal behavior. Diffuse subendocardial delayed gadolinium enhancement of each ventricular myocardium was seen. Coronary angiogram showed normal epicardial coronary arteries. A biopsy of the tongue showed deposits of amyloid substance in the sub-epithelial region. Congo red stain revealed apple green birefringence in polarizing microscopy. The patient was finally diagnosed as a case of cardiac amyloidosis, correspond to monoclonal immunoglobulin light chain amyloidosis (AL). He was then referred to a hematologist and chemotherapy with bortezomib + cyclophosphamide + dexamethasone (BCD) regimen was initiated.
Echo_Video_PLAX.mp4
Echo_Video_ A4Ch.mp4
Case Summary
Cardiac amyloidosis is underappreciated as a cause of common cardiac diseases or syndromes such as heart failure, aortic stenosis, or unexplained left ventricular hypertrophy. In developing countries like Bangladesh, diagnosing patients can be a real challenge. Echocardiography plays a vital role in the diagnosis and management of cardiac amyloidosis, especially in Bangladesh, where advanced imaging modalities may not be widely accessible.