CASE20250430_001
Transfemoral Aortic Valve Implantation Across a Tortuous S-Shaped Aorta with Severe Calcification: Technical Strategies and Outcome
By Melly Susanti, Seung-Woon Rha, Cheol Ung Choi
Presenter
Melly Susanti
Authors
Melly Susanti1, Seung-Woon Rha1, Cheol Ung Choi1
Affiliation
Korea University Guro Hospital, Korea (Republic of)1,
View Study Report
CASE20250430_001
TAVR - Complex TAVR
Transfemoral Aortic Valve Implantation Across a Tortuous S-Shaped Aorta with Severe Calcification: Technical Strategies and Outcome
Melly Susanti1, Seung-Woon Rha1, Cheol Ung Choi1
Korea University Guro Hospital, Korea (Republic of)1,
Clinical Information
Relevant Clinical History and Physical Exam
An 85-year-old female with a history of atrial fibrillation presented with progressive dyspnea on exertion, reduced exercise tolerance, and occasional chest discomfort over the preceding months. Her past medical history included hypertension and mild hyperlipidemia, with no prior myocardial infarction or cardiac surgery.
Relevant Test Results Prior to Catheterization
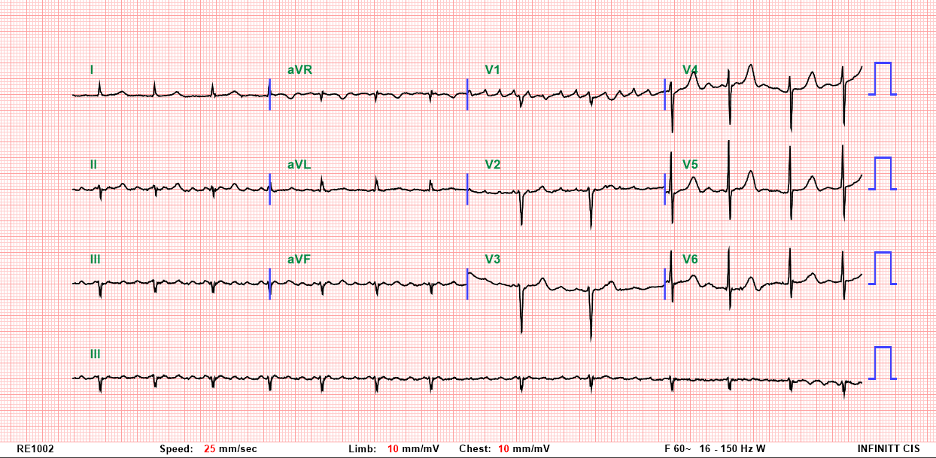
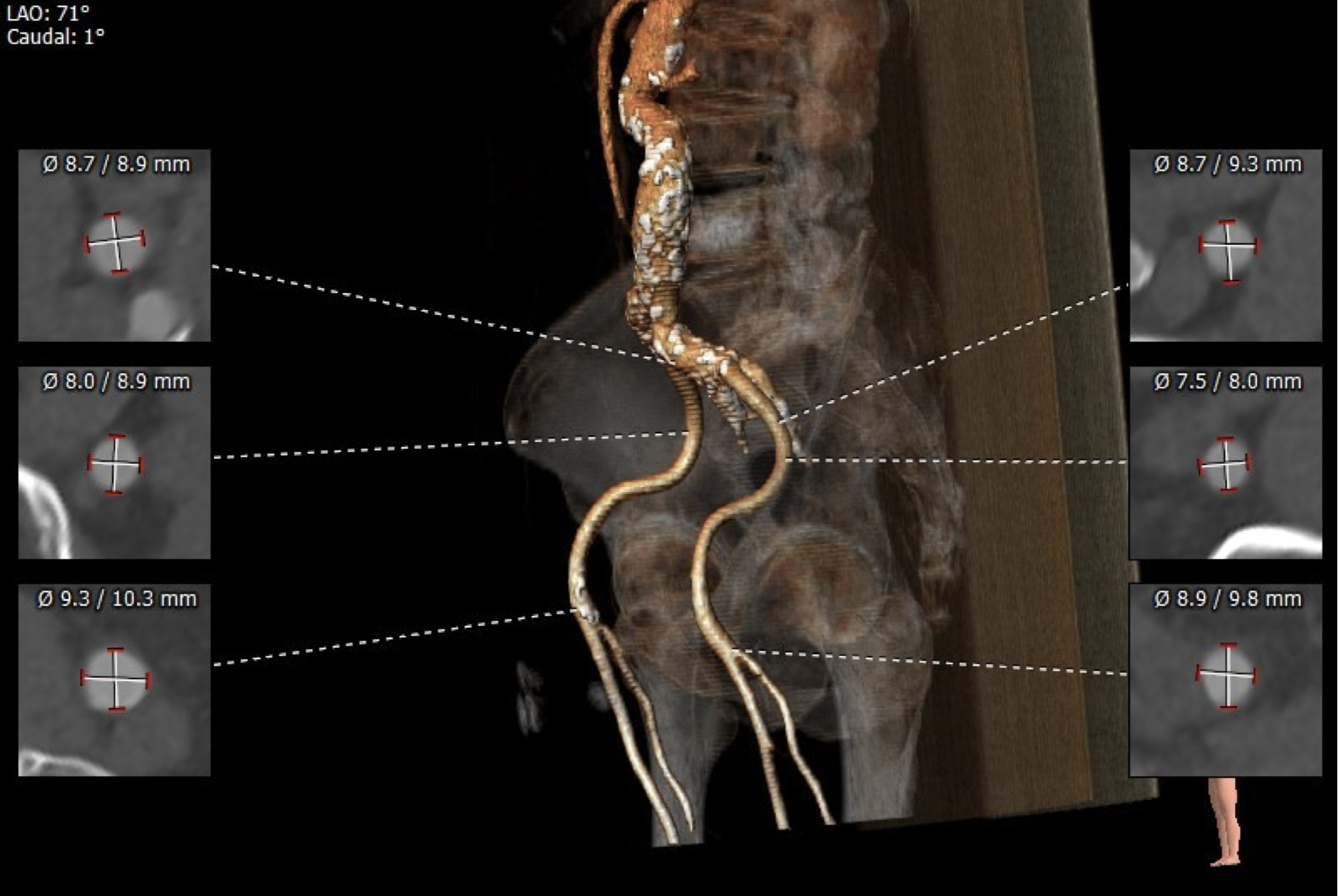
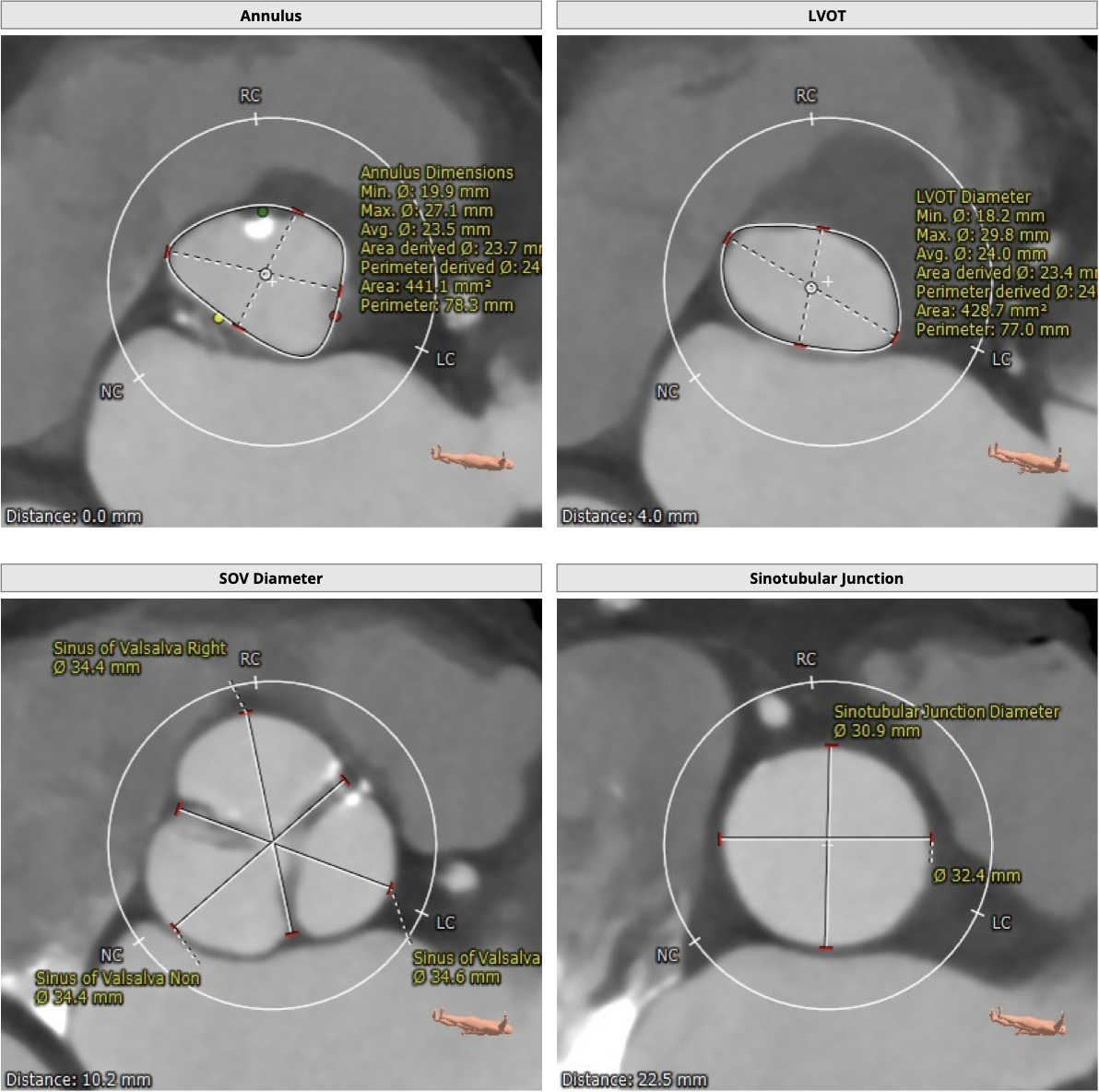
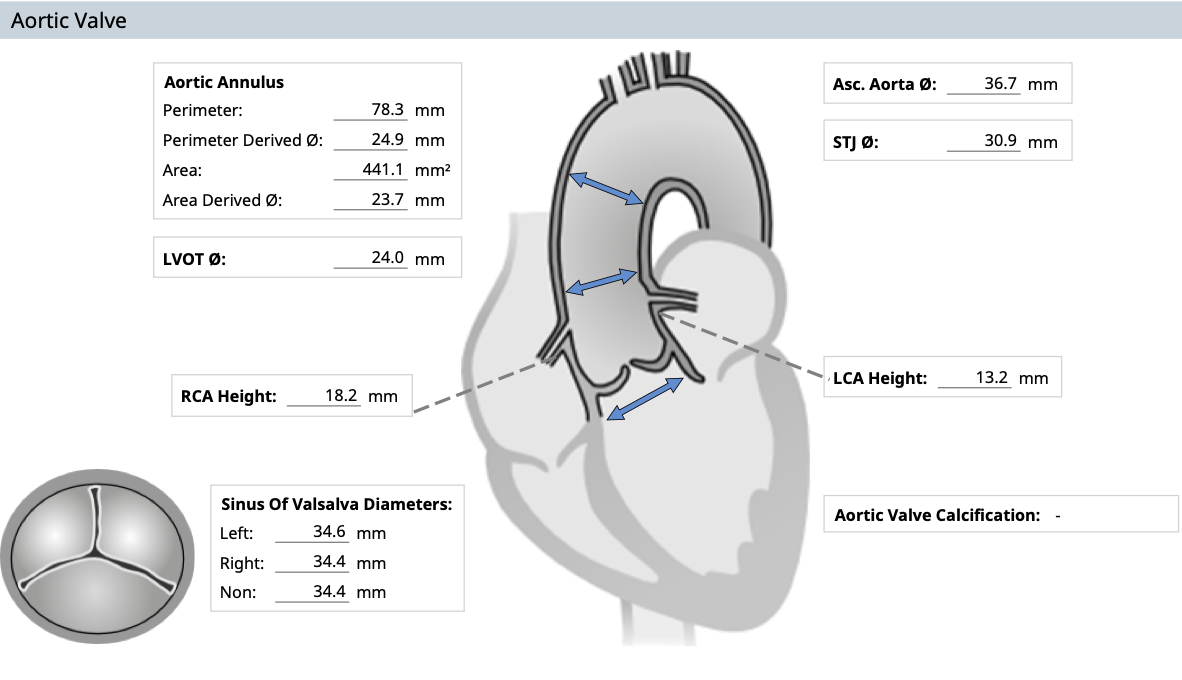
Severe degenerative AS (AVA 0.36 cm², Vmax 5.4 m/sec, PG 117/74 mmHg) with preserved LVEF (60–65%), mild-to-moderate TR, dilated atria, 43 mm ascending aorta, mild pulmonary hypertension (PASP ~43 mmHg). TEE confirmed severely calcified AV, no LA thrombus. EKG showed AF with controlled rate. Preprocedural CTA revealed severe S-shaped abdominal aortic tortuosity and calcified iliofemoral arteries, guiding transfemoral access.
Relevant Catheterization Findings
Coronary angiography showed normal left main artery and mild diffuse atherosclerosis in the LAD, LCX, and RCA. Aortography confirmed severe calcified aortic stenosis with limited cusp motion.
 aortography.wmv
aortography.wmv
LCA.wmv
RCA.wmv
Interventional Management
Procedural Step
The patient underwent transfemoral transcatheter aortic valve implantation (TAVI) using a 26 mm Edwards SAPIEN 3 Ultra valve (Edwards Lifesciences, USA). Given the severely tortuous, S-shaped abdominal aorta and calcified iliofemoral arteries, careful preprocedural planning was essential. Access was obtained via the right femoral artery for valve delivery, the left femoral artery for pigtail catheter placement, and the left femoral vein for temporary pacing. A Lunderquist wire (Cook Medical, USA) was advanced through the left femoral sheath, and in combination with an angled stiff wire (Terumo, Japan) from the right side, helped straighten the tortuous aorta and provide necessary support. An AL1 catheter was advanced over the right-sided angled wire, which was later exchanged for a soft straight Terumo wire to cross the stenotic aortic valve. Sequential catheter exchanges (AL1 → Rubicon → pigtail) were performed, followed by final wire exchange to a Safari wire (Boston Scientific, USA) for valve delivery. Pre-dilation with an 18 mm Z-Med balloon (B. Braun, USA) was followed by successful deployment of the Edwards SAPIEN 3 Ultra valve under fluoroscopic and echocardiographic guidance. Post-deployment imaging confirmed excellent position with only mild paravalvular leak.
Double wiring.wmv
Tortuous aorta.wmv
Edward was trying really hard.wmv
Case Summary
This case demonstrates that transfemoral TAVI can be successfully performed even in the presence of severe aortic and iliofemoral tortuosity and calcification. Careful preprocedural planning, combined multiwire support to straighten the anatomy, and stepwise catheter and wire exchanges were essential to ensure safe valve delivery. A multidisciplinary Heart Team approach was key to achieving optimal outcomes in this high-risk elderly patient.