CASE20250412_001
Narrow Escape from Death
By Farrukh Malik
Presenter
Farrukh Malik
Authors
Farrukh Malik1
Affiliation
National institute of cardiovascular diseases , Pakistan1,
View Study Report
CASE20250412_001
TAVR - Complex TAVR
Narrow Escape from Death
Farrukh Malik1
National institute of cardiovascular diseases , Pakistan1,
Clinical Information
Relevant Clinical History and Physical Exam
Patient introduction and purpose of procedure:75 Male hypertensive presented with Multiple episodes of Syncope since last 6 months. Clinical examination revealed aortic stenosis.Admitted for TAVR. Aortic stenosis STAGE D1. STS SCORE 8 EUROSCORE 1.7
Relevant Test Results Prior to Catheterization
IMAGING
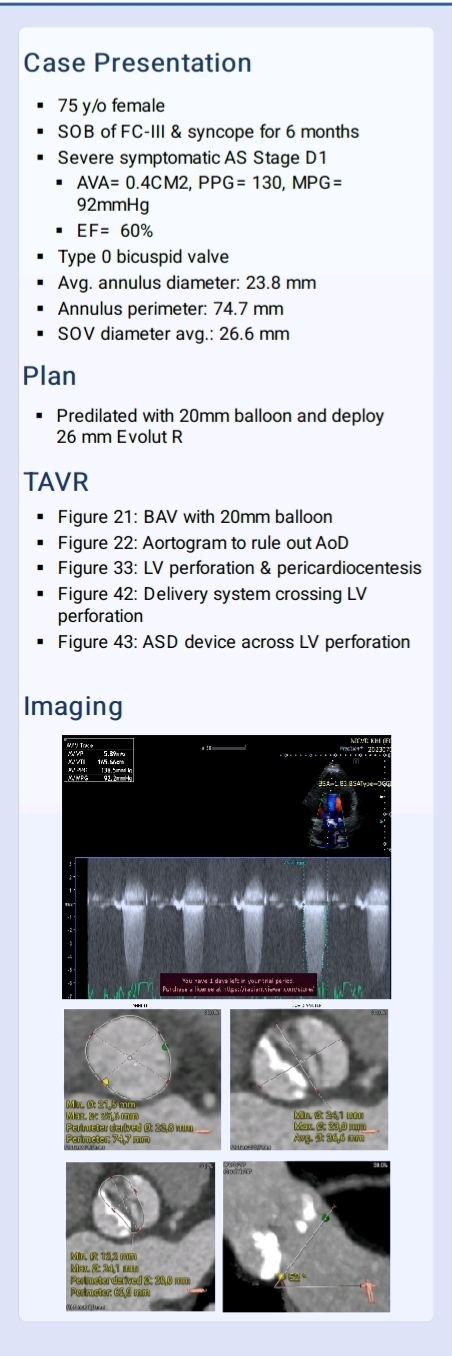
Echo findings AVA= 0.4CM2, PPG= 130, MPG=92mmHg
EF= 60%
Ct scan
Type 0 bicuspid valve
Avg. annulus diameter: 23.8 mm.
Annulus perimeter: 74.7 mm
SOV diameter avg.: 26.6 mm
Relevant Catheterization Findings
Interventional Management
Procedural Step
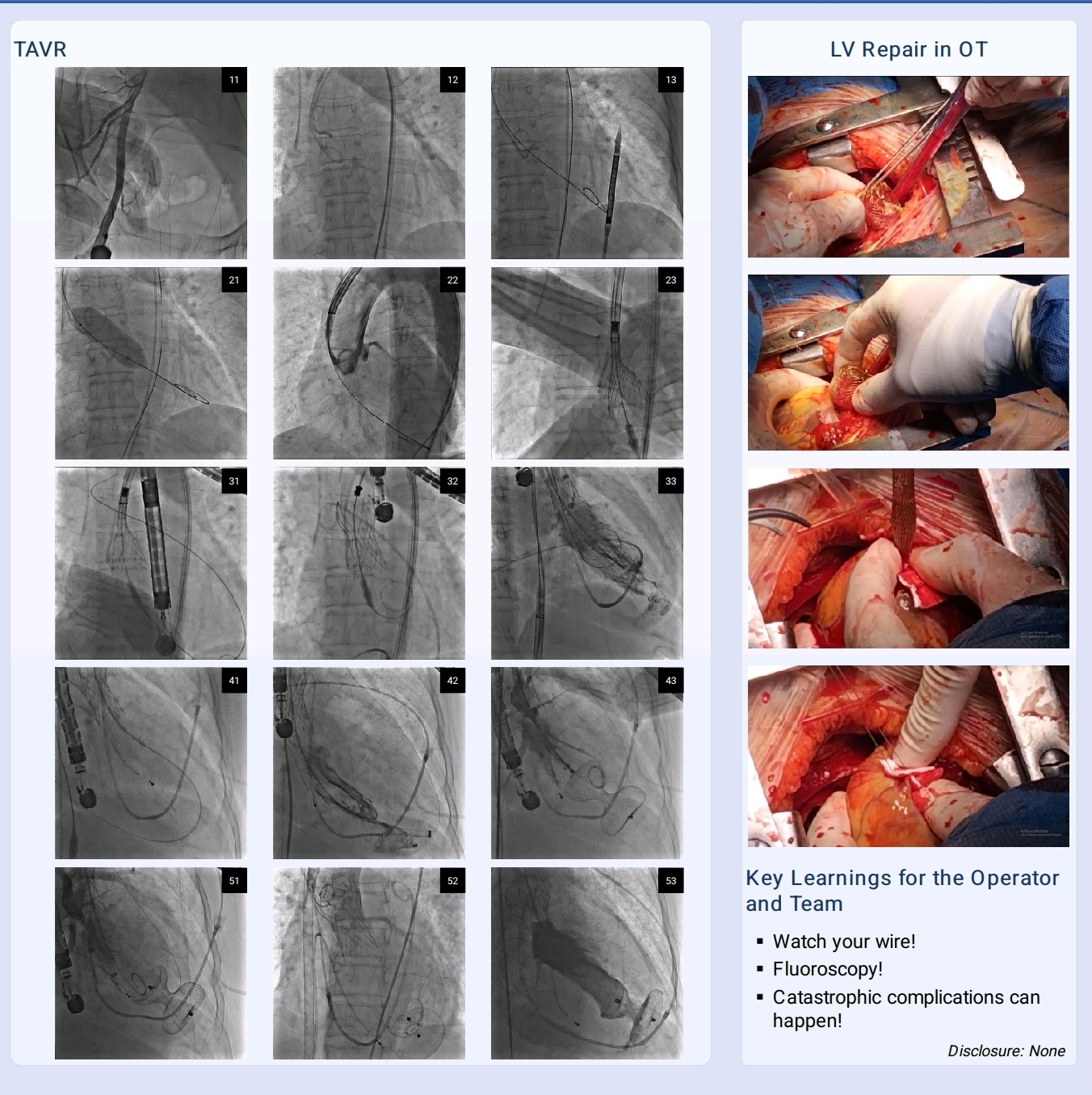
Ultrasound guided Femoral access taken under Conscious sedation . Confeida Brecker wire placed in LV. BAV done with Burst pacing. EVOLUTE Core Valve 26 delivery system loaded on guidewire and advanced. Blood pressures dropped to 60/ 40. Heart rate dropped to 30 bpm No peripheral pulses CPR started with adrenaline push. Sluggish heart activity on fluoroscopy. TEE showed rapidly accumulating effusion. Check injection in LV confirmed LV perforation by Stiff wire.Attempts to solve the problem:Percardiocentesis done during CPR. Pigtail Catheter placed in pericardial cavity. 600ml of fresh blood auto transfused. VA Ecmo passed. Device delivery sheath placed in pericardial cavity. Lv Perforation sealed with Large sized ASD device occluder.Patient shifted to OR . Lv perforation closed by pericardial patch and ASD device removed.
Case Summary
What was the root cause:Left ventricle apical perforation by Stiff wire during Tavi Valve advancementHow to avoid in the future:Left ventricular rupture occurs rarely (eg, 0.27 percent of TAVI cases) . Accounts for 18.9 percent of cases requiring emergency open-heart surgery and 23.5 percent of post-TAVI tamponade cases . This complication can be reduced by use of pre-shaped TAVI specific guidewires It is advisable to maintain strict fluoroscopic surveillance of the stiff guide wire in the left ventricle during valve deployment.